Just to fuel the Covid debate that is going on here, I offer this from the latest React Study from Imperial College London:
As they say:
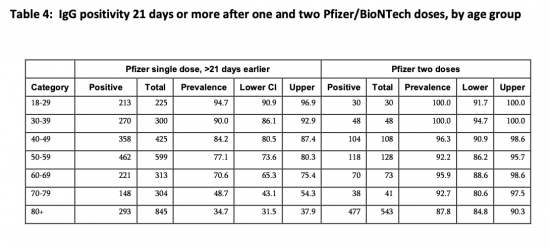
In 971 individuals who received two doses of the Pfizer-BioNTech vaccine, the proportion testing positive was high across all age groups, at 91.1% (88.5, 97.1) overall. Following a single dose of Pfizer-BioNTech vaccine after 21 days or more, 84.1% (82.2, 85.9) of people under 60 years tested positive (unadjusted) with a decreasing trend with increasing age, but high responses to a single dose in those with confirmed or suspected prior COVID at 88.8% (85.9, 91.2) overall. (Table 4) The apparent higher positivity in people with prior COVID-19 was present in all age groups.
I suggest the evidence is abundant: two doses are needed, and the sooner the better.
A single dose does not appear to be achieving anything like the expected benefits, most especially for the vulnerable.
On this basis, government policy would appear to be placing wholly inappropriate faith in single-dose jabs that do not deliver vaccination for those who really need it.
Thanks for reading this post.
You can share this post on social media of your choice by clicking these icons:
There are links to this blog's glossary in the above post that explain technical terms used in it. Follow them for more explanations.
You can subscribe to this blog's daily email here.
And if you would like to support this blog you can, here:

 Buy me a coffee!
Buy me a coffee!

I can see the UK becoming a pariah nation as the virus gets stamped out in other countries through pursuit of a zero-covid approach while Boris insists on pretending one shot (of whatever) will work when plainly it won’t. Still, elect a madman and what can you expect? I had mine yesterday, by the way, an AZ locally, one stop on the train and a short walk. What I was encouraged to do by our insane government was travel by public transport all the way across London for a single Pfizer shot. I ignored the official advice and waited till the alternative was available locally. I imagine I’ll live longer that way. These are hazardous times indeed.
Nobody is getting a single jab? Everybody is getting a double jab with an extended period in between so a much larger proportion of the population are afforded some protection sooner. The policy makes sense.
As this data shows, the delay does not make sense
Please stop lying
It is you that is lying Richard and you know it. The strategy of one dose with a longer gap before the second has been supported by experts…As published in the BMJ on 3rd February.
“Commenting on the study, Paul Hunter, professor in medicine at the University of East Anglia, said, “Taking all this evidence together, the 12 week gap between first and second dose is clearly the better strategy as more people can be protected more quickly and the ultimate protective effect is greater.”
Your refusal to publish such learned comments is telling. You are embarking on a deliberate campaign of misinformation.
One that Indepdnent Sage and others who know much more than me agree with
The government is wrong
Just stick to the facts, not democidal politics please
It’s nice of Richard to suggest that I should receive my second dose of vaccine before my 38 year old daughter, who is a primary school teacher, gets her first dose but I do disagree. She needs that dose more than I do. IMO.
Of course it would be good if we both could get a double shot quickly but this is not an option. I think we can all see both sides of the case here and so it is perfectly possible for reasonable people to disagree. Talk of “democidal politics” does seem to be OTT.
This government has killed people through its actions
Democide is the completely correct term
Do not try to excuse their behaviour – tens of thousands of people have died because of their indifference – including 1,000 healthcare workers for lack of proper PPE
If you approve of that please don’t post again.
@ Richard,
This thread is about the argument in delays of the second jab. Not about PPE and other failings of the Government last year which we all should be critical of. This time last year the talk was on letting the virus move through the population unchecked, to build up a “herd immunity”. This was entirely inappropriate. They took this line for several weeks and was largely the reason we did so badly compared with other European countries.
The government weren’t helped at the time by some poor scientific advice but they were the ones making the decisions so they do have to be held accountable. Particularly on PPE and long time reluctance to mandate the wearing of masks.
However, the question of whether I should receive a second jab before my sons and daughters receive their first is a different matter. I’d always put them first even if this means I’m “democidal” according to your definition.
With respect, there was no poor scientific advice
There was just callous decision making
You are peddling falsehoods here
I wouldn’t bother to try again – you are banned for excusing democidal policies
Dear Richard,
You are seriously unhinged!
If I was you would not think it worth commenting
Surely the right choice depends on age? If we have doses to allocate we should allocate them on the product of vulnerability and improved protection. Since the over 80s have higher vulnerability we should give them first to people who’ve had one dose as they get an extra 53% protection and then to those who’ve had no dose.
For people aged 70-79 its slightly better to give them to those who’ve had no dose – though really the numbers aren’t good enough to be sure.
Second doses for people under 40 should be lowest priority.
Actually, the spreaders probably need the doses first
Bizarrely, the case for vaccinating the young is very high because they are doing the spreading and the vaccines work best there
Doesn’t that depend on why you are vaccinating, and what other measure you take. We know lockdown cuts back transmission substantially. So then perhaps your first imperative is to protect the most vulnerable groups.
Out of a lockdown, perhaps it becomes more important to prevent transmission, and you switch to vaccinating the younger groups who are circulating the virus, and rely on the vulnerable keeping themselves safe, a la Barrington. I think the government might struggle to communicate why they are leaving the mostly vulnerable at risk under that policy.
@ Richard,
It’s an interesting argument that the younger spreaders, who probably aren’t at such high personal risk, should be prioritised over the more careful elderly who are in a higher risk group. It could be right but most people won’t see it that way.
There does, judging by the fall in recent vaccination figures, look to be a shortage of available supplies. So should we use those limited supplies to give a first dose to the younger age groups or a second dose to us oldies? I’d vote for the latter if I were acting solely out of personal interest but I do see the sense in vaccinating the younger spreaders too. In an ideal world we could do both but we wouldn’t have Covid to deal with in that world in any case.
The biggest spreaders are at work.
I go to building sites to snag and handover new properties from contractors – invariably workers are not wearing masks (some are better than others).
It’s a variable that the Government seems unaware of.
Sure – we have a lockdown in a formal sense – bit in REALITY we have gaps everywhere.
That’s where Covid continues to thrive: in the gaps created by ignorance or fear (itself produced by a lack of Government support).
Agreed
And those gaps are about to get a lot bigger
If I read this correctly, it says that for the over 70s one dose gives you a 50/50 chance of being immunised with two doses offering around a 90% chance. Is that so?
I will wait for my second jab before getting too close to my friends and neighbours!
However, in a world where vaccine supply is limited it is still possible that delaying the second dose to get more first doses delivered makes sense – although that idea looks increasingly thin for older groups.
What irks me is that what was a “make do” policy decided in the face of lack of vaccine capacity is now hailed as a triumph of British ingenuity and when I see the numbers of vaccinations delivered nightly on the news I have to check my phone to ensure that I have not been transported back to a 1950s Soviet Union news broadcast.
Yesterday I said on this blog that I thought it was possible that the unlock timetable was reasonable (bar “big bang” school opening) but that it should be flexible in the face of evidence. Well, for me at least, this is new evidence. I also read yesterday (can’t remember where) that “R” was creeping back to 1 in some areas even before lockdown eases. Against this there is preliminary evidence that suggests much lower hospitalization rates for the “single dosed old” (handily presented to us by a compliant media).
On balance, only a day on I am edging towards changing my mind and saying we are going too quick.
I think you read it correctly
It’s not quite that simple, not least because antibodies are just part of the immune response and we don’t yet know how much of an influence that T-cells and B-cells have on resistance to this infection. The Scottish study seems to indicate reasonable efficacy after just one dose even in older people so it’s a surprise that these antibody measurements seem to show much lower numbers in this group than might be expected. The chances are that there will be increased protection against serious illness a few weeks after the first dose (as the Scottish study would indicate), regardless of these measurements. All of the studies are calculated on relatively limited data at present, however, so the devil might remain in the details.
It’s also worth noting that the study on which this thread is based relates to just the Pfizer mRNA vaccine. The length and strength of duration of protection from the new mRNA vaccines are a bit of an unknown at present so it certainly is more of a gamble to space the dosing with these. Providing the first dose provides a good deal of protection as indicated in Israeli and the Scottish studies, I do think it worth the gamble. However, the duration of protection might be an issue if people have to wait 12 weeks between doses so I’d hope that those who have had just the first dose (which is still mostly the elderly and vulnerable), continue to be especially careful until the second dose is received. I certainly hope not many have to wait 12 weeks between the doses, however.
For vaccines with adenovirus vectors such as the AZ vaccine, the data shows that these provide a stronger response a longer delay after the first dose so it is less of a ‘gamble’ to space the doses with this vaccine type. We know a lot more about how adenovirus-vector vaccines operate and, indeed, the J&J vaccine which has now been approved is intended for use as a single dose (although they are also running an extended 2-dose trial as well). The data for the J&J vaccine seems to indicate that it takes 4 weeks for most vaccinees to fully seroconvert.
Ultimately, the important numbers will be the hospitalisations and deaths. Let’s hope the gamble of getting some protection into a lot of people more quickly rather than better protection into half as many works out well. Logically, it ought to. We’ll know more and also have comparisons available with other countries within a couple of months.
Hospitalisations and deaths are very important of course, but also important are the substantial number of people who suffer mild symptoms initially but develop and suffer from debilitating long COVID for months. And the opportunity given for the virus to mutate further, presented by a large population with high levels of infection and also many people with a reduced level of immunity. Addressing both of these requires us to push down infections as low as possible.
I don’t disagree, Andrew. My teenage niece has been unwell for some months with what we believe is ‘Long Covid’, although getting a specialist to look at her is pretty much impossible. She has almost completely lost her voice and has been awaiting an ‘urgent’ scan since the start of the month. No news of that as yet. However, stopping hospitalisations and deaths is of more import and the initial data for the vaccines does seem to indicate that they reduce transmission to some degree. Let’s hope that this holds true after just a single dose as well.
I suspect that we wouldn’t have seen the JVCI recommendations for additional spacing of doses of the Pfizer vaccine had the government not made such a complete balls up of things before Christmas. As soon as they knew that B117 was so much more transmissible, they should have ‘cancelled Christmas’ completely, regardless of the political fallout. The fact that the borders were closed a week before Christmas was a pretty good indication that things were very serious.
I do think the JVCI would have recommended spacing the doses of the AZ vaccine as there was some data that longer spacing between doses improved the strength of the immune response for that particular vaccine.
My wife is a secondary school teacher in her 30s so will be in a classroom full of teens most of the day. It seems a bit perverse that she’ll not be getting her vaccine until after me (I’m in my late 40s), even though I have no contact with hardly anybody but my young children and colleagues at work, most of whom have already had a dose of vaccine for one reason or another! The JVCI are just drilling down into the statistics in their decisions.
I have a young friend (the daughter of a friend, now at university) who has carried lungs and long term skin issues from Covid, caught last September at university
Really disabling
This thing is not all about the elderly
That isn’t what the study says at all!
It says that they don’t have enough data on second vaccinations yet, but the data they do have shows:
91.1% of people with 2 jabs have antibodies.
88.8% who have had one jab, but also ad COVID have antibodies
84.1% who have had one jab but not COVID have antibodies.
So they are saying that one jab gives almost the same level of protection as two. They also say that a single dose jab results in a 72% reduction in infections. and this:
The data here suggest the optimum interval may need to be tailored to population groups, with a longer delay in
second doses more appropriate for younger age groups and those with prior infection.
So basically not what you are claiming at all. Why are you doing so then?
I have fairly presented their data
It does not say what you are suggesting
It says second diesel are required fir effectiveness
Take it up with them, not me
You haven’t presented the data fairly at all.
They say that one dose provides a good level of resistance, especially among younger people and those already exposed to COVID. They also say there isn’t that much data about how much more effective the second dose is as simply not enough have been given out yet.
As I already mentioned they say a single dose has led to a 72% reduction in infections.
You say that two doses are needed and one is not enough, and one dose is not achieving the expected benefits.
You are are wrong in your claims and outright lying when you say you have presented the data fairly.
I presented their table and their words
And the data is very clear
Like many others of democidal inclination here today, you are banned
Are you looking at the same data? How can you ignore that trend? Ok the confidence is not great but even at its worst the trend is clear.
To quote from the study “In studies of individuals 80 years or over, a single dose of BNT162b2 is associated with a greater than 50% reduction in cases 28 days after vaccination, rising to 98% after second doses are given, emphasising the importance of second doses, particularly in older populations.”
So, some effect, but second doses are essential to reach full effectiveness in older people.
She is a troll
The astroturfing class are out in force this morning Andrew
To be fair, I think it is one of those issues where reasonable people can disagree as we don’t have all the evidence to make the position clear. At its best, there is a difficult balancing exercise. At its worst, we are putting peoples lives at risk.
Given we were focusing in the first instance on people aged over 80, and then progressing in 5 year groups, (over 75, over 70, over 65, etc,) and deciding between giving people one dose and then waiting rather a long time for the second, rather than giving two shots at the normal intervals, then at its simplest, the question is whether it is better to give one person full protection (say, 90%+) or two people partial protection (crudely, a lower number). If the second number is less than half the first, you have to go for two doses, and then prioritise (although working out indicative numbers is hard enough, but there is another a difficult question as to what “protection” means here: whether the vaccination stops infection and/or transmission, and/or makes symptoms less severe). There is also the interesting point that vaccinating at wider intervals can improve the immune response, but at the risk of leaving a person more vulnerable in the meantime.
For the 80+ group (about 2.7 million people) 34 is much less than 84, even taking into account the confidence intervals. For the 70-79s (4.9 million people) twice 48 is probably better than once 92, but we could have vaccinated both of these groups twice already. Instead. we are working through the 60s and down to the 50s. Which may be great for them, but not so good for older people.
What we are doing is consistent with a policy of trying to reopen as quickly as possible – single shots for everyone, and damn the consequences for those left vulnerable.
Hannah, I did not understand “Table 4” as presented; for me, it needed much more introduction. It looks as though you have read the report and do understand what those figures say.
The statement that you took from the report – this –
“The data here suggest the optimum interval may need to be tailored to population groups, with a longer delay in second doses more appropriate for younger age groups and those with prior infection.”
– seems to me to be exactly what we should understand from the study, while awaiting further data.
Thank you, for your helpful comments.
Perhaps it might be better to try to avoid being accusatory, though, despite feeling got at!
With respect, Table 4 is pretty darned hard to misinterpret
Much as I have suspected for a while, this suggests single shots work well in younger people with good immune systems, who in the main are not getting them, but work much less well for the older people we really want to protect. What we need to see are data on hospitalisations and deaths for different age cohorts, vaccinated and not.
Grant Shapps was falsely claiming last night that a third of the population have been vaccinated. 18.5 million is significantly less than a third of 66 million. But that is only first doses. Only 700,000 (about 1%) have had the second dose that is required.
Very glad to be proved wrong if new data comes through to support the suggestion today that there really is 80% protection for the eldest after one jab.
Here is the preprint PHE are trumpeting. https://www.gov.uk/government/news/new-data-show-vaccines-reduce-severe-covid-19-in-older-adults
Can someone explain how “We find that a single dose of the BNT162b2 vaccine is approximately 60-70% effective at preventing symptomatic disease in adults aged 70 years and older in England and 2 doses are approximately 85-90% effective. Those vaccinated who went on to become a symptomatic case had a 44% lower risk of hospitalisation and a 51% lower risk of death compared to unvaccinated cases. … The effect of a single dose of the ChAdOx1 vaccine against symptomatic disease was approximately 60-75% and there was again an additional protective effect against hospitalisation, though it is too early to assess the effect and mortality.”
turns into
“Combining this with our minimum vaccine effectiveness against symptomatic disease estimate, would suggest that a single dose of BNT162b2 is around 80% effective at preventing hospitalisation and around 85% effective at preventing death with COVID-19.”?
Nonetheless, if this stands up to scrutiny, clearly good news.
That is pretty weird….
I have seen such concerns on Twitter too…..
Perhaps it is taking the whole age range into consideration, not just over 70s?
So the study says that people with previous infection do well with one injection. I had quite severe CV19 at the very beginning of the pandemic (all recovered now) but since the NHS was not able to test me at that point (this was early March last year when they were totally overwhelmed), they have no record of my infection, even though I got it confirmed with an antibody test – they will not acknowledge the result.
The NHS seems to have a policy that they only trust their own data – so for them I have not had CV19 – and that is regrettable. I did get my first Pfizer shot and would be happy to skip the second one for now, but there is no process for that in place. I do not know how many shots that would free up but I think it would be significant.
Thanks for your good work Richard!
Just to be clear, the table you show is reporting the presence of one type of antibody (IgG) in vaccinated individuals. IgG levels are the most common marker used to track an immune response, but they aren’t direct evidence that those individuals are protected (or not) from infection.
The best data is from the real world, which is now emerging. The Israeli data gives little indication about protection from a single dose, but the emerging data from the UK (Scotland) does. In the unreviewed paper released on Monday, at 4 weeks from a single dose there was 85% protection from serious infections needing hospitalisation with the Pfizer vaccine and 94% with the AstraZeneca vaccine (https://www.bbc.co.uk/news/health-56153600). Obviously since vaccinations only started in December for Pfizer and January for AZ there is no way of getting longer term data other than wait for the next analysis.
You make the interesting point that maximum benefit might come from vaccinating those most likely to spread infection. Everyone is hoping vaccines stop transmission, but there is currently little evidence for that – by which I mean it isn’t yet known, not that it doesn’t happen. There was a small subgroup in the AZ clinical trial (and also a similar one in the recently reported Janssen trial) that suggests Covid vaccines do reduce transmission but only partly, so far less effectively than prevention of severe disease. Once again, we just have to wait for real world data, and no one has reported convincing effects yet for either Israel or the UK.
There are very good reasons to doubt the Scottish paper – not least the very short survey period
True, one would like longer data from Scotland and I am sure updates will be available in time. But with AZ vaccination only starting on 4th January, there couldn’t really be much data on those over 4 weeks from vaccination at an analysis point mid-February.
It would be nice to be able to fast-forward to see what happens next – that would transform vaccine immunology! (Economics would find it pretty convenient too). But sadly the real world in real time doesn’t work like that.
If it interests you, I was alerted today to a new paper showing prevention of asymptomatic as well as symptomatic disease following a single dose of the Pfizer vaccine. Which implies that it would be stopping transmission which is what everyone wants to see evidence for. Again, since these were vaccinations following regulatory approval they necessarily cover a fairly short period. https://www.authorea.com/users/332778/articles/509881-single-dose-bnt162b2-vaccine-protects-against-asymptomatic-sars-cov-2-infection?access_token=-hDTQsMUXcCPSpdZV_Lmpg
Its always been a political campaign rather than a public health emergency, including daily headlines dictated to the compliant BBC. Obviously the ‘world-beating’ single dose headlines too tempting not to go for. Beeb rarely if every mentions how many actually fully vaccinated. Johnson & Sunak took a deliberate decision to kill tens of thousands by rejecting the science on 21 September, and are now setting out to kill tens of thousands more on their route map , so a few more thousand deaths of only partially unvaccinated is neither here nor there.
Don’t forget the ‘T’ cells – though I’m not sure what difference they make overall- that’s a different study, and possibly more difficult to do.
Since the “perverse” Covid virus strategy is to hop from as many individual recipients as possible those who mix together whilst travelling on a regular basis and on the basis of their daily activity have to communicate a lot with others are the ones the Covid virus “enjoys” meeting. Since the elderly although highly vulnerable to being killed by the virus and not in nursing homes tend not to be in the above category spending greater time at home being retired would suggest a more thoughtful strategy than automatically saying elderly first and then working your way down to the youngest for your vaccination policy.
Do anyone using published information from academic or clinical sources which suggests an improved overall outcome (in terms of hospitalisation sir deaths) for delaying the second jab is now deemed “democidal”.
In the same way anyone who voted to leave the EU was deemed a “fascist “and “racist” by your good self.
It’s little wonder you spend most of your time writing a blog instead of carrying real influence as you appear unhinged at time’s.
Thank you Sarah
I note your dual trolling identity
And if I was so irrelevant you would not be trying so hard to get on here, as you clearly are
You can’t even make your own case
Transmission risk and vulnerability beyond the elderly ignored by the JCVI who don’t appear capable of a multi-faceted analysis of the Covid problem:-
https://www.independent.co.uk/news/health/covid-vaccine-priority-groups-age-jcvi-b1808178.html
In the announcement of the vaccination “Phase 2” this evening – delivering first doses to another 21 million people aged over 18 by the end of July – did I miss the bit when they said when they would complete delivering second doses to the millions of the most vulnerable people who were vaccinated in December and January? Have they set a target date?
According to the dashboard, still under 750,000 second doses have been given so far, mostly done before 10 January. Just a reminder, over 2.2 million first doses had been delivered by 10 January. By 31 January it was 9.2 million, and today it is 19.2 million. There are about 9 million people aged 70 or over.
On 25 February, 485,000 first doses were given, and 35,000 second doses.
I did not hear it- but am told the JCVI says it is happening
I suppose it depends on how close to the 12 week gap they are willing to stretch. It’s not 7 weeks since the 10th January as yet, so you could theoretically expect that this date gives you a few weeks to give 1.5 million second doses well before even a 10 week gap. It’s obviously not helpful that we’re told to expect a temporary dip in number of doses given during much of March as both the Pfizer and AZ vaccines are encountering production delays which are expected to be resolved before the end of the month. Assuming the reports of coincidental shortages in both vaccines aren’t just smoke and mirrors to hide a redistribution of doses around Europe.
I also don’t understand the reluctance to prioritise teachers and the police, in just the same way as NHS and care home workers. I appreciate there has to be a limit (what about prison officers, public transport, retail workers, food processing factories, plumbers, …) and I understand they are not thought to be at increased risk of hospitalisation or death, largely I suspect on grounds of age, but if we are asking these public sector workers to put themselves at risk we should be protecting them before 40 year old bankers and lawyers and accountants and consultants working at home. In this case the politicians hide behind the scientists, but as the saying goes, advisers advise and ministers decide.
I hope they do have clear plans for second doses. I am one of the lucky ones who have had their first dose (age 65-69) and at the time was given an appointment for my second. As have an awful lot of others. News items suggest one of the reasons for the hiatus in vaccination rate over the last week has been the need to start stockpiling for second dose appointments (especially with the Pfizer vaccine which is itself going through a supply drop due to them reconfiguring their manufacturing).
I think some of the commentators here don’t realise how extraordinary it is that we are even discussing second phase rollout of already approved vaccines just 14 months from first designation of a new infectious disease. We would all love more data, and in particular longer time series, but the expectation has been set by previous vaccines which had been years in their trials and development. Science may have moved fast on this one, but the human immune system still follows its normal timescale.
We simply do not have the evidence to say whether the Government strategy of delaying the second shot was right or wrong.
I think that on balance it was the right decision, and as an 80-year old with one Pfizer jab I have a vested interest. Richard thinks otherwise.
There is no point in any of us using emotive language. Any decision will cost some lives and save others.
Both the Scottish study which suggested good protection of over-80s and the REACT study suggesting less protection are preliminary, we need to wait for more data.
Two definite points:
– IgG is a useful marker, but it is only part of the protective effect of vaccination
– When generating antibodies in the lab, delaying the second dose generally gives better final antibody production.
I look at the Government COVID data every day. Two things to look for
If vaccination of vulnerable groups was working, after a lag you would expect deaths to decrease faster than new cases. This has been the case since February 11th.
Less encouraging, although new cases are still declining, the rate of decrease has been slowing since the start of February.
Both may of course be blips.
Thanks
“— When generating antibodies in the lab, delaying the second dose generally gives better final antibody production.”
Delaying it for how long though? There must clearly be a point beyond which levels fall or else we’d all, for sensible reasons, be on one jab.
At the end of the day, it makes little difference [what is said here].
Under-18s are not being vaccinated, there is no data yet on use of either Pfizer or Astra (or any) CV19 vaccine in that age group (although trials have started). That age group is around 20% of the population.
Vaccine uptake in the higher-age group is good, over 90%.
Vaccine uptake in the minority communities is, not that good. Estimates range from 57% to 70%.
Vaccine uptake in the illegal migrant community is zero (estimates of the size of that population range from 300,000 to 1.2 million).
Currently, with the current vaccine uptake figures realised, it will be barely possible to reach the herd immunity threshold.
I doubt there is any current plan to vaccinate-by-demand, so there may well be a permanent base of infection.
There is a large social media base of disinformation and outright lies on the vaccine. Ranging from “it contains trackers to follow you” to “it sterilises you” to “it’s just to kill coloureds”. And worse: “the mRNA vaccine programs your DNA to self-destruct after a few years”
I consider that an extended second dose regime is the least of the problems; currently.
The initial lack of PPE was at least partly caused by the failure of the privatised emergency store, where it was found that so much kit was out of date and unusable. That is not specifically down to this corrupt, incompetent and evil crew, though it can still probably be laid mainly at the Conservative’s door. Have we been told of any intention to set up a proper and well maintained emergency store, based on lessons which could be learned from this pandemic, ready for the next one?
They were warned of this
And they are still a Conservative government
You also utterly ignore their reaction to this
What is this willingness to excuse democide for? It happened
Here in Australia where there is no need to protect people fast using the vaccine ( as we’re protected by NPIs), the regulator has just approved the AZ vaccine for doses 12 weeks apart. This because the data show its most effective that way. Getting the second shot sooner is worse. Specifically for AZ.
Is there any such thing as ‘the data’? Surely there’s only ‘data’ and different data will provide different results according to who are compiling it, doing the testing, the nature and accuracy of that testing etc? We need really to be able to view and interpret a wide variety of data in order to be able to make any kind of assessment for ourselves, and I’m afraid we really aren’t getting that.
By “the data” I mean the data available to the regulator, which is more than is made public. Here there is quite widespread belief in the regulator doing what’s best. Of course political pressure plays a part, but as I say, there is little pressure to move fast, so I think 12 weeks is a fairly neutral position.
I despair of people like you
Sorry, it ha to be said
The quietly compliant are what make government irresponsibility possible
You demonstrate repeated ill-informed comment on things you know precious little about. The evidence re vaccination is increasingly clear that the UK approach is the right one. On what basis do you know better than the scientific advisors that have advocated this approach that is more and more supported by evidence day by day. Your voice criticising this approach is a classic example of someone overreaching their expertise to offer (irresponsible and ill-informed) public opinion. Good academics know when they can add to debate and when to stand back and leave space for those with more expertise but you seem – sadly – so arrogant as to assume you know better than this those with considerably greater expertise. You have no expertise in immunology after all so why do you think it appropriate to offer an opinion on things you know absolutely nothing about?
This is not an academic blog
It is my opinion
I discussed the vaccine situation with a hospital consultant today. Three things came out:
a) Pfizer is in very short supply
b) No open wants AZ if they know anything about medicine
c) The hospital group he is in is preparing for the next wave in Jul;y, but admit that it could be earlier as a result of new variants.
I use sources to form opinion
You are just offering abuse
Interesting. Can you cite the geographic area the consultant works in and their expertise?
a) I’ve been told (by one of the vaccinators) that our local mass vaccination centre has 2 weeks of Pfizer in stock, with occasional dips in supply as expected.
b} What evidence is there for this claim? The NHRA, EMA & various other regulatory bodies around the world have declared AZ safe and recent reports show 90%+ performance & a 12 week gap between injections is recommended.
c) Could you identify the Trust so this can be checked?
You may of course be entirely correct – however given the position we are in I think supporting evidence for your claims is a reasonable request.
Of course I am not disclosing my sources
That’s not what is done
I have simply reported, in the way newspapers do
I do suggest newspapers are asking
My clue is start in what might broadly be called the south east of England
Graham,
I had the Oxford AZ jab, my wife was luckier and had the Pfizer.
I wish that I could have had the Pfizer, because we are told that it is more likely to be successful against the new variants – preferably given as the manufacturer recommends!
Evidence – none scientifically proven as far as any ordinary citizen knows.
What we ordinary citizens do know is that this crew of Conservative politicians are significantly less believable than the ordinary run of politicians. Setting up a Downing Street department of propaganda is evidence that the importance of controlling the story far exceeds any wish to be transparent. We DO NOT believe the spin exiting Johnson’s mouth. The only World Beating thing he has achieved is the UK’s death rate! Why should I not try to make up my own mind?
“b) No open wants AZ if they know anything about medicine” – no open what?
No one…sorry