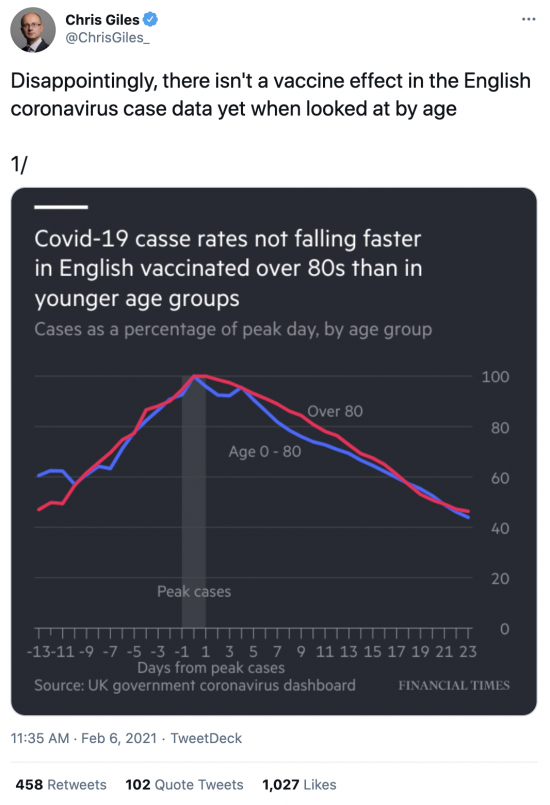
Chris Giles at the FT and I are not always known for agreeing with each other, but he is clearly onto something with this thread:

As yet this is not evidence that the government's policy of delaying the second dose of vaccine (and no-one is vaccinated until they have it) is wrong. But right now it does not look good.
We will know more in a couple of weeks, but if the data does not then being to look like that in Israel, which is giving second doses in three weeks, then the policy will very clearly be wrong.
We need to see a 'vaccine effect'. If we don't all the celebrations, and all the reopenings should be put on hold as another failure would have to be marked instead. And I admit, that is what I suspect is on the cards.
Thanks for reading this post.
You can share this post on social media of your choice by clicking these icons:
There are links to this blog's glossary in the above post that explain technical terms used in it. Follow them for more explanations.
You can subscribe to this blog's daily email here.
And if you would like to support this blog you can, here:

 Buy me a coffee!
Buy me a coffee!

It is a high risk strategy with an optimism bias built as usual.
We are assuming that single shots deliver significant benefits in older people by extrapolation from how vaccines and viruses “ought” to behave, but without much specific scientific evidence. As far as I am aware we don’t have much good evidence that any of the vaccines work well (in preventing illness and death) with a single shot and then a second one three month later. We don’t have particularly good evidence for the vaccines working well for older people, particularly with a single shot strategy. There is not much evidence on whether vaccines prevent transmissibility rather than just illness and death. Israel is doing well but they are well into second shots.
We’ve been vaccinating since December so we should have getting on for two months of evidence from the natural experiment we are running. Where is the evidence then? How are we doing? How are vaccinated cohorts doing as compared to others?
The NHS had done well in delivering the first shots, but we need to move rapidly to delivering 10 million+ second shots. We must get the virus under control to reduce the risk of another variant emerging that evades the vaccines.
UK cases are down significantly due to lockdown, not due to vaccinations. Hospitalisation are down a little but still terrible. Deaths remain high. There is a long long way to go if we are not to repeat the mistake of December in unlocking when ceases remain at a high level.
I really really hope we get this sorted out this year but I fear there are going to be further unwelcome bumps along the way.
I share your pessimism
Another wave is quite likely with this policy
There is grounds for optimism reading the results of trials produced by Astra Zeneca and published earlier this week..
“… AstraZeneca is safe and effective at preventing COVID-19… more than 22 days after the first dose. Results demonstrated vaccine efficacy of 76% after a first dose, with protection maintained to the second dose. With an inter-dose interval of 12 weeks or more, vaccine efficacy increased to 82%.”
^
https://www.astrazeneca.com/media-centre/press-releases/2021/covid-19-vaccine-astrazeneca-confirms-protection-against-severe-disease-hospitalisation-and-death-in-the-primary-analysis-of-phase-iii-trials.html
Now read today’s Astra results….
Although this government’s performance, and that of its predecessor, give much reason to be wary of downside risk, I’m not so much as pessimist as a sceptic. Doubt lies at the heart of the scientific method; as the motto of the Royal Society has it, “Nullius in verba”: that is, “take nobody’s word for it”. Just show me – and the rest of us – the evidence, please.
I very much hope they have got this right, because the alternative is awful. But without a firm evidence base, it is essentially a gamble.
A very high stakes on too
You can read the pathology of the disease here. Then appreciate the difficulties:
The four horsemen of a viral Apocalypse: The pathogenesis of SARS-CoV-2 infection (COVID-19)
https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(20)30262-0/fulltext
# ohnM says:
February 9 2021 at 7:27 am
Yup. Been there, done that.
Difficulties now appreciated. Thanks.
(Gulp!)
We are barely into 1 month since vaccinations started. The manu info is that second doses be administered after 21 days Pfizer and 26 days Astra.
There will be little data coming in yet, and none of the vaccines promote antibody production in under 14 days. And locally, peoples children of teenage years and up are still socialising. A group of 4 having a meet-and-drink session were fined £800 each (some people won’t take heed of prior warnings!). People are still allowed into the country from hotspots. Hotel quarantine is still a gleam in some tory hotel-owners eye. Why should the govt care, they’re saving a fortune in benefits are creaming-it in fiddles.
No matter how bad things are, there are always people getting rich off it.
It is probably too early to come to any firm conclusions as yet. The fall in UK cases for the over 80s is similar to what we have seen in Israel for the over 60s. The curious thing to observe is that there doesn’t seem to be the same fall in cases amongst the younger cohort in Israel.
But there are differences. Israel has given at least one dose to a far higher percentage of its population than the UK so we are probably around 3 -4 weeks behind them. Wind back the Israeli data by the same time and there is little sign of their vaccination program having worked.
But if we don’t see some positive results ourselves in the next month or so we should reconsider our one shot approach to vaccinations.
I said this is early data
But the absence of any similarity already is worrying
And this needs to be watched
That is as far as I cam going
If you vaccinate care residents first, which are cohort 1 after all, then you would expect to see outbreaks in care homes coming down as a proportion of the total. The data on this from Public Health teams comes with a lot of caveats, but over the last 3 weeks they have indeed come down.
But that has not been UK policy
It has been Scottish policy
Scotland has made care residents slightly more of a priority in England, that is true. But in England they have not been ignored. Care residents in England are still classed as Cohort 1 – and while the data on respiratory outbreaks in care homes from Public Health teams comes with a lot of caveats, over the last 3 weeks they have indeed come down in England as a proportion of total outbreaks.
Mz Hurst,
Scotland has simply followed JCVI advice closely (as advised), and effectively completed first dose delivery to elderly residents in care homes, before systematically cascading down the priorities, according to best practice. This is because the programme of care home vaccination is slower and more resource intensive than for other groups. The plan allows for an acceleration in coverage once care home results are delivered; because they provide the highest protection against the death rate. They had 98% first dose delivered by last week in Scottish care homes (and for practical/technical reasons that is effectively 100%). These are just facts. More facts on vaccine delivery would have been given, but the British Government objected to the Scottish government publishing them. Please note that publishing these statistics would allow the UK Government priorities to be factually monitored.
The UK Government has been coy about care home vaccination levels in England; it gave a figure last week of 90%+, for those “offered” a dose in care homes. This was deliberately ambiguous. The figures reained opaque, and the UK Government tried to attack the Scottish Government’s vaccine delivery, while refusing to provide (or allow publication of) the facts about vaccine supply (variously under the guise of commercial sensitivity or national security), all the while spinning a story of Scottish failure to the UK press, and the need to bail Scotland out, while suppressing the facts.
Alex Thomson, C4 News however managed to produce a figure for English care home actual first dose vaccination last week. This evidence seems to be all we still have in the way of facts on coverage in England; that should give everyone pause for thought before forming an opinion. Thomson’s figure for English care homes by last week was, incidentally circa 80%.
@John S Warren
Is there any reason you know of why PHS hasn’t published data on ARI outbreaks in care settings and total ARIs, so that a weekly progression can be worked out. I’ve looked and cannot find one. It would be re-assuring to know that the vaccination programme is working in all parts of the UK, and that Scotland with it’s higher proportion of single dose delivery is doing just as well if not better.
And please don’t call me Mz, thank you.
Sarah Hurst (if I may),
“Is there any reason you know of why PHS hasn’t published data on ARI outbreaks in care settings and total ARIs, so that a weekly progression can be worked out.”
The Scottish Government published the stats on vaccine supply (as part of the ‘four nations’ agreement on coordinating policy), on grounds of transparency around two weeks ago; and the UK immediately demanded the withdrawal of the data. The Scottish Government complied, but under protest. The UK Government then immediately began briefing the media with a story critical of the Scottish vaccine roll out plan, claiming it was slower than rUK, although the Scots followed closer to the JCVI advice (initially slower to reach the wider public, but the more effective strategy on public health grounds of protecting the most vulnerable first). Public health officials who know what is happening in Scotland generally approve the success of the roll-out. The UK government, and Scottish Unionist politicians brief otherwise. The Scottish government late last week aid that given such tactics being adopted by by the UK government, it will simply publish the stats. This is where we are, as best I understand it.
You tell me why this is happening.
Cat-Pigeons
” ChAdOx1 nCov-19 provides minimal protection against mild-moderate COVID-19 infection from B.1.351 coronavirus variant in young South African adults”
https://www.ox.ac.uk/news/2021-02-07-chadox1-ncov-19-provides-minimal-protection-against-mild-moderate-covid-19-infection#
Mind you since most vaccines don’t prevent you being infected, it is a moot point! Very few vaccines are sterilising vaccines.
Just repeating same mistakes as last year – with all the same self congratulatory hubris about how many millions tested/vaccinated etc. and no clear strategy – beyond the implied ‘living with it’ and ‘culling the old’ .
Some of us, Independent Sage – Sir David King etc have consistently been advocating getting infection down near zero and keeping it there – with a properly functioning Find, Test, Track, Isolate, Support system which could quickly detect and eliminate local outbreaks – as in several Eastern countries , NZ, Australia etc.
No sign of a rethink despite the 112,000 deaths, the second dose fiasco, and inevitable variants resulting from continuing high levels of infection. This will doom us to continuing ducking and diving, restrictions and possible further lockdowns.
‘Freedom loving’ back benchers seem to have no inkling of, or desire to understand, how this works.
The main way of stopping endless infections was, and is, immunity gained “by heard”. Vaccination would be nice, but unfortunately vaccination against RNA virus has not been a success story in the long term.
The best way of gaining a form of herd immunity is to let the virus run wild. As was the policy at the start. Then it was policy after the start, and is still policy now. The rolling lockdown policy is good at deflecting blame in various directions, the vaccine rollout deflects blame in other directions, it’s almost inevitable (if partial) failure will deflect the blame away from politicians, and towards the organisation that will, inevitably, be blamed when control is finally gained over the virus: The NHS. If you cannot see the NHS being blamed and becoming the fall-guy, you are far too innocent.
Look at the history of this, and consider that the govt *will* have been aware of which countries in the present and past have controlled the spread and the ways they did it. Think: SARS1 & MERS (and all other communicable disease).
Since the press is owned by the same people that own the Con-Servative party……………………
People are too trusting.
Got my part1 vaccination done. The side effects were a bit harsh. S’life.
“heard” should be “herd”
Herd immunity is only a tactic if you have given up on elimination. Elimination can virtually be attained if the borders are closed; as with Taiwan. Britain still hasn’t closed its borders. It appears to have decided it doesn not wish to close its borders, or is incapable of doing so.
Britain voted through Brexit to take control of its borders, so that it could fail to take control of its borders. This is polict in 21st century Britain.
When it comes to elimination it is easy to overlook the Isle of Man which receives relatively little press coverage compared to locations such as New Zealand and Australia.
Of course it is a small jurisdiction, but this has been achieved with closed borders, and huge amounts of effort going into test, track and trace. A traditionally conservative (with a small c) jurisdiction it has imposed very substantial restrictions on civil liberties for the relatively brief periods that have been necessary to eliminate the virus, not once but twice. The UK has pussy footed around with fines which started out at incredibly nominal levels whilst the Isle of Man judiciary has typically handed out 4 week prison sentences for breaking any self-isolation or lockdown rules. This sort of punishment will always focus minds in ways that a fine will not, and when you are risking the lives of others in the community it is perhaps not an unreasonable measure.
The Isle of Man is rarely celebrated on this forum, but in this particular area it has to be said that they have done a very good job of eliminating the virus and providing residents with a normal life. The Isle of Man is often described as a boring tax haven with nothing to do, but right now you can do more in the Isle of Man than anywhere else in the British Isles.
Do you have links to data rather than assertions?
Well there is no lockdown in the Isle of Man right now, that is a fact.
The borders have been largely closed in the Isle of Man since late March 2020 (and between March and July 2020 even residents struggled to return to the island), that is a fact.
Roughly 60 people have gone to prison (typically for 4 weeks) for breaking the lockdown or self-isolation rules, that is a fact.
Which facts are you looking to ascertain, or which assertions are you looking for proof of?
Are you looking for proof of the assertion that prison is a bigger deterrent than a fine?
Maybe this link is of use … https://covid19.gov.im
You claim facts without proof
I was only asking for links…
You might find this link to the Reuters Fact Check team useful:
https://www.reuters.com/article/uk-factcheck-isleofman-idUSKBN2A42GW
On the other hand if you want a really good idea of the difference between the UK’s approach and the Isle of Man’s these links may make interesting reading:
https://www.bbc.co.uk/news/world-europe-isle-of-man-55938484
https://www.theguardian.com/world/2020/aug/23/three-jailed-isle-of-man-breaking-covid-quarantine-rules
https://www.bbc.co.uk/news/world-europe-isle-of-man-54360825
https://www.bbc.co.uk/news/world-europe-isle-of-man-55725729
https://www.bbc.co.uk/news/world-europe-isle-of-man-55280466
https://www.bbc.co.uk/news/world-europe-isle-of-man-54266517
https://www.bbc.co.uk/news/world-europe-isle-of-man-55758764
https://news.sky.com/story/covid-19-social-distancing-scrapped-as-isle-of-man-lifts-restrictions-12205197
Thank you
Really interesting
# Andrew Broadbent says:
February 7 2021 at 1:07 pm
Yup, absolutely right. I would add to FTTIS being one pillar of the solution, another would be proper awareness of the importance of VENTILATION in reducing transmission.
See here:
https://www.erinbromage.com/post/the-risks-know-them-avoid-them
reserch as known at May 6th 2020. So why are we not tackling the impilcations? Government guidance to employers re ventilation mis PITIFUL
and here:
https://fivethirtyeight.com/features/how-to-make-indoor-air-safer/
Ventilation means AIR CHANGES – not a fan on a desk! or an open window!
The bunch of charlatans running the UK government have consistently followed a high risk strategy for which ordinary citizens are the ones who actually bear the consequences. This high risk strategy goes back to the start of the post GFC period of austerity. All this high risk strategy is designed to serve the interests of the financial elite, the rentier class. The neanderthals on the Tory back benches just cannot tolerate the lockdown and a baying like wolves for “re-opening the economy” so that the rentiers can resume the normal levels of rent extraction. The last thing they want to see is a debt jubilee which becomes increasingly possible the longer folk cannot pay their debts, rents, mortgages etc. Re-opening the economy is the only way that financial obligations have any chance of being enforced to the fullest extent. Alas I think the debt problem is now way past a solution without either a jubilee or debt restructuring across the board. The plank these charlatans are walking is getting narrower but they can’y be seen to turn back so the strategy gets riskier and riskier. Government applause of our dear Captain Sir Tom Moore is just a fig leaf for their complete dishonesty. I can hardly bear to watch the news these days – I get so bloody angry. My new telly is at high risk of a boot through the screen.
Many thanks in advance
The UK vaccine stock level over time?
I have tried to find out but no success.
“To lie like a government bulletin”. I have been screaming repeatedly at everyone to get access to the data (whatever the topic with this bunch of charlatans) but with little effect. For example one can find information on average port clearance times at CALAIS but obviously not at Dover. Impossible to plan without good data, but who cares?
Single Dose Administration, And The Influence Of The Timing Of The Booster Dose On Immunogenicity and Efficacy Of ChAdOx1 nCoV-19 (AZD1222) Vaccine
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3777268
Hardly an unbiased paper, was it?
Some interesting comments there. Such as the relatively poor performance of the Oxford/AZ vaccine in older (55+) compared to younger age (18-54) groups, perhaps 30% lower immune response; the small numbers giving large error bars; and essentially no impact on asymptomatic infections, which probably means there is still a significant population able to infect others.
That paper appears to be suggesting that it may be more effective to give the Oxford/AZ vaccine at a 3 month interval. Which begs the question, why didn’t they seek regulatory approval for that regime in the first place? (I may have this wrong, but isn’t it generally the case that, all things being equal, the relative effectiveness of a vaccination increases over time anyway, as more people in the control group are infected?)
And back to the start, when are we going to see the impact of the vaccine on hospitalisations and deaths? If we have vaccinated the most vulnerable categories, and the vaccines are as effective as hoped, when should we see the effect? Next week? The week after?
Given the rapid spread of the variant which came to light in Kent, and the evidence available from the trials, it was a sensible decision by the JCVI to recommend getting a dose of any vaccine into the most vulnerable. I’m no fan of this useless government, but they really were ‘following the science’ in regards to the advice from the JCVI.
The point here is not just whether one dose of a vaccine will stop the most vulnerable becoming infected, but rather, in the event that they do become infected, they suffer from less severe illness. The evidence from the trials indicates that all of the vaccines greatly reduce the risk of severe illness (and I’d hope that this will be true with the South African/South American variants as well). Giving twice as many vulnerable people a lesser degree of protection will almost certainly reduce the number of deaths in comparison to fully vaccinating half as many people.
It is very frustrating that no data is being released about the severity of infections at present (and this problem of a lack of data is true in all countries around the world). In theory, the rollout of the vaccines should hopefully reduce the proportion of infected people who require treatment in hospitals and therefore also reduce the proportion of those who die – at least, this is what the trial data showed. I’ve had a quick search but can’t find a breakdown of the age ratio of those who are admitted to hospital for treatment. The number of hospitalisations is falling as you would expect given the lockdown, but it isn’t clear if this is faster or slower than would be expected. This would be one of the first places where the numbers would begin to change, providing the single dose does protect against severe illness. Hopefully the comments about a potential increase in virulence of the UK variant aren’t correct as it is bad enough that it is so much more transmissible.
It may be that the Oxford/AZ vaccine is less effective than the others but the situation here is that a dose of a slightly less effective vaccine now is likely to be better than no vaccine at all with the hope of getting a dose of a better one a couple of months down the line. The US is doing it by the book at present, following the Pfizer/Moderna two dose regime and there are increasing calls from many in the scientific community over there to get a single dose into as many vulnerable arms as possible, especially as the more transmissible UK variant is beginning to spread over there.
The comparison with Israel is fine, as long as you take note of the differences between the programmes in the two countries. By the end of 2020 approximately 10% of Israelis had received their first dose of a vaccine and they were targetting vulnerable groups in exactly the same way that we have been. At that point, we were still well below 2% vaccinated. Israel have a deal with Pfizer to rush through the vaccination of as many people as possible in return for sharing of data. As the UK population is around 7 times that of Israel, there simply wasn’t enough vaccine around to match their rate back in December and early January and still isn’t. Even with our rapid increase in vaccinations during January and February, the Israelis have given more than three times as many doses per capita of a vaccine as we have. It also appears that it takes over 3 weeks for the immune response to really kick in with the Oxford/AZ vaccine so there is that delay to consider also.
I’ve read that the scientists hope to see an improvement in infection numbers by the end of February but it would also be helpful to know if the ratio of severe illness in those vaccinated is beginning to fall. The fact that no such information has been even mentioned (i.e. whether there is or isn’t an apparent effect), is very strange to me.
Some more good news from Israel hopefully.
‘A new coronavirus drug which successfully cured 30 cases of the disease in Israeli hospital patients has been hailed by scientists as a huge breakthrough’.
https://uk.news.yahoo.com/israeli-covid-drug-cured-30-191709659.html
I’m sceptical about numbers given in a vacuum without a proper trial for such treatments. Hopefully, this treatment will be an effective one but no way of knowing for certain without proper randomised trials. If the Israeli vaccine rollout is as effective as hoped, they’ll probably need to run such trials somewhere else!
There is something called the precautionary principle.
At every stage in the Covid outbreak, the government has ignored it.
And so far they have been wrong every time.
The good news is that something odd is happening. We can all see for ourselves that this lockdown is not being observed anywhere near as well as the first one imposed last March. The traffic on the roads now is much greater than it was then. Many, especially younger people, have lost all fear of the virus and have had enough of being cooped up at home. We have new strains appearing which may be more harmful and probably more transmissible. As the OP says there is no real indication from published data that the vaccine program is starting to have the desired effect.
Yet, in spite of all this, the infection rate has fallen sharply, and continues to fall, by around 70% from its peak of a month ago. I don’t know anyone who predicted it would be so sharp. It will be some time before we know the reason for this. It is possible there have been many more natural infections than is generally known, and so more induced natural immunity has built up in the population. I know from my own fortunate experience that Covid can be ultra mild. It is often easily missed especially if we are expecting a far more severe illness. Incidentally I would have missed it myself had I been 100% truthful, in the on-line application for a test form, about my symptoms. The computer would have said no! That I did not need a test.
There does seem to be some room for cautious optimism. Especially if the mass vaccination program, albeit with delayed second doses, does start to have some measurable effect, even if it is not quite what we all might be hoping for.
I think you are looking through rose tinted specs
As ever your criticism is politically motivated more than any understanding or appreciation of the science behind it.
Is that true of the FT?
If nit, why not?
The rapid rise and fall of the Covid Gompertz curve is highly seasonal. Israel just doesn’t have N European seasons, so it’s curve will behave differently.
Oh come on……
I think everyone expects too much!
In 2017-2018 the average effectiveness of the flu vaccine was 15% overall (27% children to 17, 12% 18-64 and 10% 65+)
In 2018-2019 the childrens was 87% effective, the adults to 65 was 39% and the over-65s’ was not given, but I thing it was about 20%.
The next season the adjuvanted trivalent inactivated vaccine was used for the antiques and resulted in a higher effectiveness of 60%.
The problem with vaccines is that the vast majority do not come anywhere near 100%. And with older people whose immune systems are of decreasing ability, 60% was excellent (although some countries in Europe have been using the adjuvanted vaccine since 1997 !!)
And that is with a well-matched vaccine. New strains throw things right out.
I don’t expect the Pfizer vaccines 95% to be replicated in real-world conditions. I had the Astra vaccine in preference, because the mRNA vaccine is too “novel” and has no usage history to refer to. The Astra is more conventional. Time will tell.
People seem only to remember vaccination as the end of smallpox, in fact it was a large part of it, but the reason smallpox was defeated may sound familiar:
“It was fear of these kinds of epidemics that encouraged developed countries to fund the smallpox eradication campaign. Seven years after it had been proposed the campaign began in earnest in 1966 with the appointment of DA Henderson. Although mass vaccination calmed fears, it was not always the most medically efficient way to combat the disease. Henderson and his team developed a strategy of containment and surveillance. Every time there was an outbreak, a WHO team would arrive, vaccinate and isolate those who were ill and trace and vaccinate all their contacts. Effectively they ring-fenced the disease until it had no way of moving on to its next victim”
https://www.bbc.co.uk/history/british/empire_seapower/smallpox_01.shtml
Vaccination is a large part of the fight…..but behaviour modification is also a large part.
It isn’t working well in the states, where social distancing is regarded as denial of freedom by many. 475,975 deaths to date. And the UK and Brazilian variants are now starting to spread stateside.
12 million plus, first doses.
500,000 plus, second doses.
First vaccination was on 8 December, if I remember right.
And the disparity is the problem, politically created
It’s 4 weeks since the vaccinations started, so if 12 weeks was the strategy no second vac should have been done.
Remember I said the NHS would be blamed? Here are your IEA friends
https://m.huffingtonpost.co.uk/amp/entry/institute-for-economic-affairs-nhs-nothing-special-myths_uk_6021b667c5b6c56a89a3b4ed/?__twitter_impression=true&guccounter=1&guce_referrer=aHR0cHM6Ly90LmNvL0R1ejhta0QycWU_YW1wPTE&guce_referrer_sig=AQAAAE8JmiIeaLrkJToFDwbwbep8kwc-HanE9VsDzugqU9PThxcA5rLYk_VcVJ35WColL4qfJEAI0K1ieUqmx1oPAJG0xLQRvV3bdFkL5lFVcgxqCvXnIa0jarJ9X0O-s5zM4NYslFGfqoKUWsu1ThMN-HxOlE64-dYUVVObWsfD7u1-
Intrigued by how many doubters here (almost conspiracy theorists). Happily my background is much better in biology than economics (in which I am just a curious reader) and it needs to be said loud and clear that the UK strategy is actually very low risk.
Different manufacturers aren’t working with different human immunology, and all the current vaccines target exactly the same spike protein of the virus. There is a theoretical question of the new mRNA vaccines behaving slightly differently, but the JCVI had the reassurance of Moderna data about that. So the vaccines are likely to be closely similar in their response to new variants and the longevity of the primary immune response (apparent differences are probably due to non-comparable clinical trials). There are risks with any new vaccine but not much different risk with the interval between doses; by far the biggest risk is not vaccinating people at all.
I don’t seen this as a biological issue, it is a philosophical one (some would say political). Do you go for the maximum proven benefit for the few, or the greatest good for the greatest number? The answer shouldn’t be hard.
I have to disagree
First, very clearly the vaccines are nit substitutes for each other – as the evidence shows
Second, there cannot be indifference to second dosing since risks vary greatly between people in the population. As a result fully vaccinating some is likely to have much higher impact than partially vaccinating many.
Well, it appears COVID deaths are coming down at last, slowly, whether due to the vaccine or lockdown or a combination of the two. It would be interesting to see how that breaks down into age cohorts: are the one who have had the first shot doing much better?
The 7 day average is still above 800 per day, and has still been 400 or more each day for three months, as we have gone from 49,000 to nearly 114,000 deaths. (To put this in context, there are about 620,000 deaths in the UK each year from all causes, or about 1700 per day, so 800 per day adds an extra 50% to the usual rate, and is 400 per day add an extra quarter to the usual rate. In a normal year, dementia and heart disease are each responsible for about 15% of all deaths so about 90,000 each.)
There is still an awfully long way to go before COVID deaths are in the low tens each day like they were last summer.
About 30,000 hospital beds are occupied by COVID patients, out of about 120,000 in total across the country.
Positive tests are still falling but slower and we might reach a steady state of perhaps 10,000 to 15,000 per day. If the death rate is 1% or less that might be barely acceptable.