The FT has reported today that:
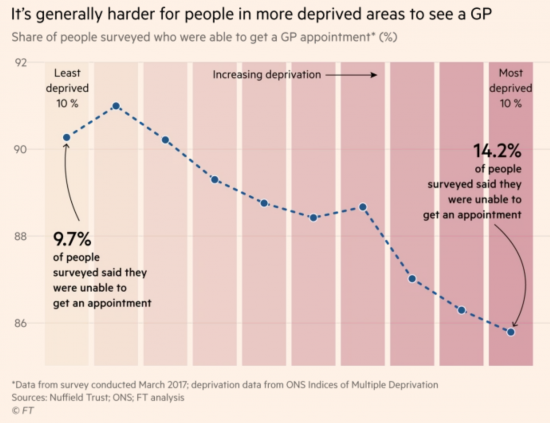
Rich and poor people in England receive different standards of care from the UK's universal free health service, with some poorer communities being “left behind” when accessing GP services, according to data analysed for the Financial Times.
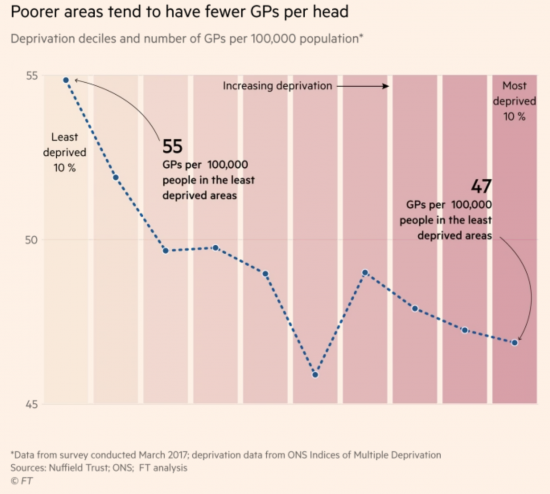
This is their data, as they summarise it:
And the explanation is not hard to find:
As I would also add, based on personal knowledge, once the second trend is in place it becomes increasingly hard to recruit because workloads are so much higher for those GPs who do work in such places.
What to do?
Differential pay would be a start. I can see no reason why not. It would only reflect workload.
Thanks for reading this post.
You can share this post on social media of your choice by clicking these icons:
There are links to this blog's glossary in the above post that explain technical terms used in it. Follow them for more explanations.
You can subscribe to this blog's daily email here.
And if you would like to support this blog you can, here:

 Buy me a coffee!
Buy me a coffee!

I’d go for a more radical solution. Putting GPs through medical school is very expensive. Analyse the job actually done and skill needs and train appropriately. My guess is many people could do a good job with an intensive post 25 course.
JohnM says:
Quoting.
“…..You’ll usually be trained to a minimum of degree level….”
When I see this my heart sinks. We’ve lost it completely now, I think.
We do not train to degree level; we educate to degree level. Or at least we used to. Increasingly, professionals are very poorly educated …just trained. If we aren’t there already it is only a matter of time before a degree is no more than a piece of paper which is paid for and is in effect a licence to practise, but offers assurance neither of competence, nor of education.
At this point the marketisation and finacialisation of our society will be complete. At which point we revert to the default currency of the free market which, as I have frequently observed, is violence.
Many practices now use Nurse Practitioners in consultations instead of General Practitioners.
The use of Physician Associates is also widespread.
“You’ll be a graduate who has undertaken post-graduate training and you’ll work under the supervision of a doctor. You’ll be trained to perform a number of day-to-day tasks including:
taking medical histories from patients
performing physical examinations
diagnosing illnesses
seeing patients with long-term chronic conditions
performing diagnostic and therapeutic procedures
analysing test results
developing management plans
provide health promotion and disease prevention advice for patients.
Most physician associates currently work in general practice, acute (internal) medicine and emergency medicine”
“Senior practice nurse/nurse practitioner
You’ll be an experienced practice nurse with a focus on working with patients with long term conditions and providing preventative healthcare to the local community. You’ll provide aspects of care previously carried out by GPs.
You’ll usually be trained to a minimum of degree level. Training would cover consultation skills, physical assessment, diagnosis, safe prescribing, research and health promotion. Your role would span aspects of nursing and medicine enabling you to treat the patient appropriately.
Some nurse practitioners/senior practice nurses with specific training and education provide minor illness and/or telephone triage services. You’ll work collaboratively with the general practice team to meet the needs of patients, support the delivery of policy and procedures and provide leadership as required”
“Advanced nurse practitioner
As well as providing the care that a nurse practitioner is able to offer, advanced nurse practitioners (ANP) will have a prescribing qualification and master’s level training. A qualified ANP is also able to:
take a full patient history
carry out any physical examinations
use their knowledge to identify a likely diagnosis
request appropriate tests to aid diagnosis (blood tests, x-rays, scans)
refer patients to an appropriate specialist (in the practice or hospital)
prescribe medicines and non-medical treatments
arrange follow up and ongoing management”
So you’ll see that GP stand-ins are available, but the minimum amount of training they need has been quantified long ago.
At hospitals many healthcare assistants do things like taking blood samples etc…
JohnM says:
“Many practices now use Nurse Practitioners in consultations instead of General Practitioners.”
In some practices you do well to get beyond the initial consultation with the receptionist.
From personal experience an established practice does well to employ nurse-practioners, call their position what you will. It seems the GP head-count can be reduced, the cost is time and effort in selection of n-p candidates, organising / division of tasks, ensuring patients understand and are happy with the ‘new’ arrangement, ensuring quality delivery of service, etc. I can say, as a patient, where all this works it works very well.
Differential pay is a good idea.
There is already precedent for this in Australia where doctors have long been scarce in rural and remote areas. It does however seem that the incentives have not been strong enough to have the full desired effect. Doctors won’t tend to go if the quality of public health services is of a much poorer standard as that makes their job so much harder.
https://www.abc.net.au/news/rural/2015-05-12/budget-rural-doctors/6464938
So, another indicator of how poverty and austerity hurts people and reduces the quality of life. A better cure is to end austerity and the need to have ‘poor areas’ in the first place and get some bloody MMT in action.
As shocking as this is, this item is doing the rounds in the Guardian and has got me really angry:
https://www.theguardian.com/education/2018/dec/29/exam-reforms-boost-private-pupils-in-race-for-universities
As the father of a Year 11 girl, I can testify to the pressure being heaped upon on her but it seems that if she were in private education, she’d have an easier ride!
Whether poorly provided health care or being put through the mincer that are GCSE’s these Tories are bastards who have a lot to bloody answer for. Bastards!
I was also really angry about this
GCSE pressure is already enormous and growing. And some can opt out. But not those subject to rule by Gove
As a diabetic I find the conversations go like this.
Me (on phone to doctors surgery in December): Can I have the first available appointment for a diabetic review please?
Receptionist: End of March ok?
Me: I guess.
Early March
Receptionist phones: The sister has left so we’ll have to reschedule – end of June ok?
Then the GP writes when June one is also cancelled saying you should be having these reviews several times a year. Sort of not knowing how their own surgery is operating.
7 years ago when I first moved to my current address (Islington, near Archway) and only had occasional minor health problems, it was normal to get an appointment at my GP practice within a couple of days. At that time there were 6 full time doctors. Now that I have a couple of long-term autoimmune conditions so need to see a doctor more often, they are down to 4 GPs (2 of them part-time), and patients are lucky to get an appointment in under 3 weeks. They do have half an hour set aside each morning for ‘urgent appointments’ (of 5 minutes) where patients can walk in and ask to be seen immediately, but the assessment of whether the matter is truly urgent is left to the receptionist, which means explaining the symptoms in public to somebody who isn’t medically trained.
I know….it’s not good
There is a long history of things not being good, through as many variations of ideological politics as you care to recall.
When I sat my 11-plus there were 46 in my typical baby-boom class – you had to be clever or damned lucky to pass, yet my older cousin was born during WW2 and it was argued that he and one or two neighbors passed their 11-plus by virtue of the need to fill the grammar school classes.
If you look at the demise of nationalized railways in the UK you see the dark shadow of Dr. Beeching with a mighty axe that destroyed thousands of jobs and community lifestyles. But what would have happened if the unions and politicians had succeeded in saving those jobs and communities. Yes, we would have had a fairer society, one seen to uphold many of the Socialist principles that have over the years been apparently eroded by the exploiting nature of Capitalism. But for how long -eventually the railways would have had to adapt to the modern era, or the pace of the UK economy would have been left behind by rivals; and so probably would our standard of living.
What then would we be saying about an NHS that had arguably become increasingly reliant on advances in treatments and medical science that had to be imported abroad. raise taxes?, create fiscal deficits?.
So, by all means laud the superiority of MMT economic logic over mainstream neoliberalism, but the measure of success is not measured in ideological preference but in practical results.
Let’s have more of the practical solutions and less of the ideological eyeballing. That latter betrays a measure of naivety.
We have the nurse practitioners JohnM mentions. They are great but need more ‘power’ to prescribe and refer. Professions generally serve the poor badly and we steal doctors from abroad already. These Tories are evil but I think we need to look at new ways to break professional boundaries to get needed work done. If you grow up poor even your brain changes differently.
Referring back to our ‘guests’ last night New Year’s Eve – they were complaining that there youngest son had an old ear complaint resurface and had been told that the treatment (around £1000) had been withdrawn like such a lot of low demand treatments in the NHS since I think 2010 if not before.
The mother had been advocating on behalf of her son like any good Mother would but I wondered if they would still vote Tory next time? Given what they told me about their feelings for Corbyn and Labour it seems that they would. You could say ‘Well – tough!’
To sum up, this family have not long moved into a very expensive house which needed a lot of work doing on it – their outgoings are huge with two growing boys and the man and wife are about the same age as me and will be entering retirement age still paying for that house. They moved because the house is more isolated and has a huge garden. If they had not moved to expensive property, £1000 for their child’s ear would have been affordable say in a private hospital (perhaps more expensive?).
Why am I mentioning this? Well because it seems that in the pursuit of a dream (a big house in the country) the family are financially stretched and things like health care and tax are contentious issues for them because they see tax in particular as competing with their other outgoings/commitments (mortgages, kids, utilities, debt, house upkeep).
I wonder how widespread these attitudes are? That some/many are anti-tax, anti-state because they see it interfering with the financing of their aspirations?
The issue over the son’s hospital treatment is redolent of what we see in the USA where people are opting out of healthcare because there is simply not the money to pay for it (low wage growth) and it is now getting to the stage that the State has to step in (Obamacare RIP).
In the UK the state under the Tories has and is stepping out of healthcare so to speak in a wage economy that although is growing is not doing so at the rates before the 2008 crash and austerity.
Looking at it through the eyes of our guests all people will see is a state that continues to takes its money through tax/NI but is also cutting back on services (as in the case of the ear treatment mentioned above).
This helps to create an anti-statist sentiment which working alongside the distrust of any political alternative (anti-Corbyn, anti-Labour) that just creates a merry-go-round of misery.
The merry-go-round grinds on slowly being vulnerable to picking up things like UKIP and BREXIT. This to me is the perverse and cunning logic that we are living with today.
It’s a nightmare.
My husband was recently diagnosed with locally advanced prostate cancer. He was referred for tests by a nurse practitioner (no complaints there) but when he wanted to talk to his GP about his diagnosis, there was no GP available… ever! For us, gone are the days of knowing or even having a GP. We are offered a nurse practitioner or nothing.