I spent some of the weekend in the company of doctors. The subject of some conversation was pretty predictable.
One doctor present said his hospital had been on red bed alert every day last year: they had never been out of acute shortage. That same doctor said this was going to get worse: closure of wards to which the hospital was committed was going to cost up to 400 bed spaces in his hospital by 2019. The replacement wards, which will have fewer beds, have not begun as yet. As he put it, rocket science was not required to work out that an even greater crisis was looming.
And we do not have many hospital beds in the UK. The last data seems to have come from 2011. I have used summaries from FullFact:
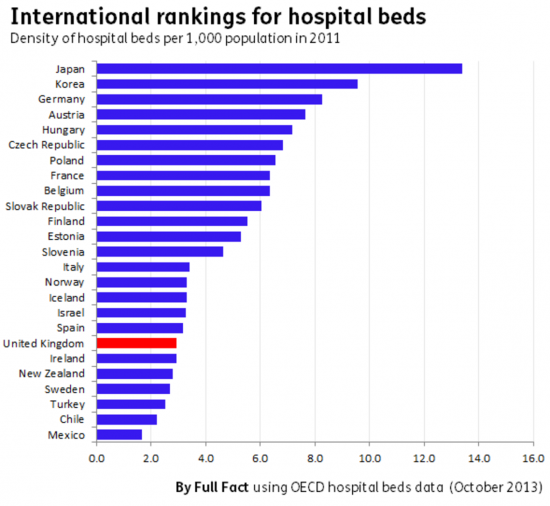
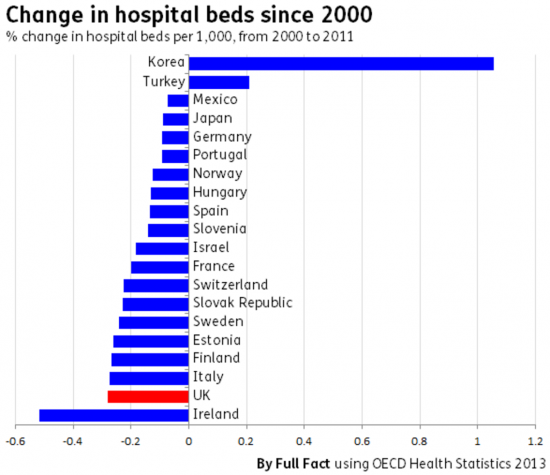
Only Sweden and Ireland are below us in the EU. And our trend is also serious:
The government says the NHS does not need more money. It says the NHS must instead become more efficient. and it is talking care in the community. But if that's the direction of travel it is moving into uncharted medical territory. Or we might instead say its taking unprecedented risk with people's lives because, like it or not, some conditions and illnesses do need to be monitored in hospitals. No one wants to be there longer than they have to be. But to pretend that we can seriously cut the hospital bed rate in the UK looks like management consultant and not medical consultant speak. And that's pretty worrying. Not least, it seems, to doctors.
Thanks for reading this post.
You can share this post on social media of your choice by clicking these icons:
There are links to this blog's glossary in the above post that explain technical terms used in it. Follow them for more explanations.
You can subscribe to this blog's daily email here.
And if you would like to support this blog you can, here:

 Buy me a coffee!
Buy me a coffee!

All areas are required to develop Sustainability & Transformation Plans (STPs) to identify how NHS is going to save @22 billion.
Apparently- they all seem similar formulae- this will be achieved by:
* focusing on prevention- shame Public Health budget will continue to be cut year on year and Government undermines efforts- e.g. watered down obesity strategy
* more care in the community – but more staff cuts! (more hidden from headline view though)
* reduction in beds …
* concentrating specialist services i.e. cuts to local provision
* focus on mental health – but cuts in funding to continue
* APPs to help you mange your own care, and support from volunteers!
* make better use of Pharmacists – but reduce the number of pharmacy’s!
None of these is achievable – we are now entering fantasy land
Except people will die as a result
It is a recognised fact that the NHS needs 4% extra a year to cope with ageing population and medical advances. The last Labour government achieved that and more, although the financial crash provided a bit of a setback. The tories have completely ignored this and are only promising 1% extra a year. Simon Stevens needs to be taken outside and shot for taking the dosh and ignoring this fact and promoting the lie that £22bn savings are achievable. And it should never be forgotten that the LibDems helped to force through the disastrous Health and Social Care Act.
Believe you me I will not forget the Lid Dems and their connivance with Cameron Carol. Their card is marked.
Sorry, but things move on PSR
The evidence has to be sought that they learned from their mistakes
NHS reductions is one thread of Tory plans to destroy public services (the peoples’ “wealth”) for the purpose of increasing private wealth. Simple.
In the meantime May and Co spool out stories (False News) of the great new things they will do for the public – today, the re-hashed promises to ‘fix’ mental health (MH). A good start would be to eliminate many of the underlying causes in today’s chaotic world; desist from the aggro to those requiring benefits. There is a fine line between surviving in life and tipping into MH illness, the road back can be long and getting help – too be honest is often not worth the effort except for the most serious. This GOVT is “world leading” in polices that send many into mental health unnecessarily. Perhaps we should mention Doctors, many are required to work before first-light to midnight. No golf course business networking or fatboy lunches in Roux at Parliament Square; for them only thoughts of tidying up the day’s lists, getting to the 7-11 in time for some food and then likely to continue on-call. No time for a Life.
What is plan B for our doctors, especially our precious juniors doctors who are not surviving? Mr Hunt it is time for your HExit.
There’s an old anecdote about a couple of ancient Greek philosophers arguing about how many teeth a mule has, only to be told by a third man that a mule has x number of teeth. “How do you know?”, ask the philosophers. “I counted them!”, is the reply.
This isn’t really fair to the pre-Socratic philosophers such as Herakleitus and Parmenides, but it’s the point eloquently dealt with by one of your commentators, who did a long post on computer coding, and how it was far too often done indigenously – ie, within the programme – rather than endogenously, by seeing how the programme was implemented, and operated on the “shop floor”.
This, of course, is why, when I was working in the small HQ Organisation & Methods team of a big IT and telecoms company we were so dismissive of ISD – Information Systems Division – exactly because they often failed to start with the user and what he or she was trying to achieve, and started instead with the system, and tried to get it to do what they thought it should be doing.
Alas, it would seem these NHS management “experts” (funny, isn’t it, that Gove never railed against the snake-oil merchant management-speak “experts” of the private management consultancy jungle: there are real experts out there, but you have to search really hard for them) seem to fall into the same category of not only ISD, but of even Main Board Directors (with whom I engaged quite often, as we were HQ O&M), who blithely informed me that he expected to see a “year on year 10% productivity improvement” by using IT.
10%, year on year!!! Alice in Wonderland stuff, which, if achieved, would mean one man would end up running a whole factory that had previously employed hundreds. An average 2% to 3% over 10 years, maybe, but 10% is an initial one-off, followed by 3 or 3 years of minimal, or only very modest, productivity improvement, gearing up to a new 10% leap after maybe 5 years.
That’s the world these management consultants should be living in, and even then they should be factoring in the 4% increase in funding that Carol Wilcox correctly referred to.
Alas, I fear they all live in this self-contained fantasy land, where such productivity improvement and savings can be achieved.
Even worse, the individual to whom I made reference above, the Main Board Director, when on to chair a government Review into savings across the public sector in 2004/5. Needless to say, I was not persuaded by the outcome! You start with the user and his or her needs, and build up your proposals from there, and NOT from the position of desired savings, which it the basis upon which these abysmal STP’s are predicated.
Starting with user need?
Absolutely.
But the problem is that the Tories are also employing an assessment of user need with the aim of not meeting it at all, thereby manufacturing consent to ‘change’ it and bring in more private business I’m afraid to improve returns….ooops – sorry – improve the service…………apparently.
The new NHS is sweating the assets – and they include the staff – and being marketised with abandon. In markets the customer is supposed to be king.
It turns out that the customer is the government in general rather than the particular patient whose need requires to be met.
A very odd sort of market.
In fact no market at all.
May P
Hmmm……..
The customers will be the financial sector, management consultants, lawyers (of course) and eventually investors and their accountants when the Tories have done reeking havoc.
So we have a health system with one of the lowest levels of beds per head of population, and the lowest cost as a proportion of GDP. At the same time it delivers (or used to) some of the best health outcomes, as described in the Commonwealth report of a few years book. Any rational analysis would see that as evidence of a highly productive and efficient health system.
When any system becomes overloaded, it can end up spending more time scheduling and rescheduling its scarce resources than it does doing useful work. In the computer world it used to be called thrashing. That sounds to me a bit like where those massively over-burdened hospital staff and managers are today
Hunt and his advisors show no understanding of the basics of operational management or O&M that Andrew mentioned
Agreed